
Case Result: $6,000,000 Settlement — Bilateral Subdural Hematomas, Skull Fracture, Traumatic Brain Injury
A pedestrian was struck by a vehicle while crossing legally in a crosswalk with a green light. He suffered bilateral subdural hematomas that expanded on repeat CT imaging, a skull fracture in three places, an intracranial bleed, and a traumatic brain injury requiring ICU admission. I recovered $6,000,000 for him and his family.
A subdural hematoma is one of the most serious and life-altering brain injuries a person can suffer. Blood accumulates between the brain and its protective outer covering, building pressure against brain tissue that can cause permanent damage, coma, or death if not identified and treated quickly. When this injury is caused by someone else’s negligence — a car accident, an Uber or Lyft rideshare collision, a fall on dangerous property, a workplace incident, a bicycle or pedestrian knockdown — you have the right to recover full compensation for what was done to you.
I’m John J. Roach, a San Francisco personal injury lawyer with extensive trial experience. I have handled subdural hematoma and other serious brain injury cases arising from car accidents, pedestrian collisions, bicycle accidents, slip and falls, and other traumatic events. I understand the medicine behind these injuries, I work with the right medical experts, and I know what it takes to prove the full lifelong impact of a brain injury in court.
If you or a family member suffered a subdural hematoma because of someone else’s negligence, call me at (415) 851-4557 for a free consultation. I work on a contingency fee basis — you pay nothing unless I recover money for you.
What Is a Subdural Hematoma?
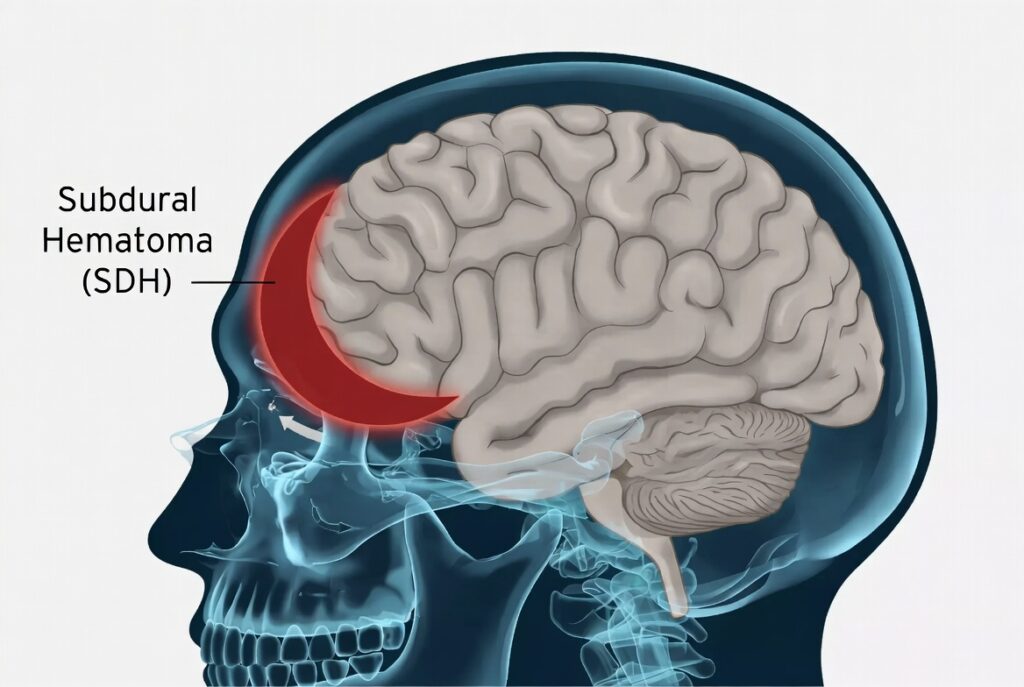
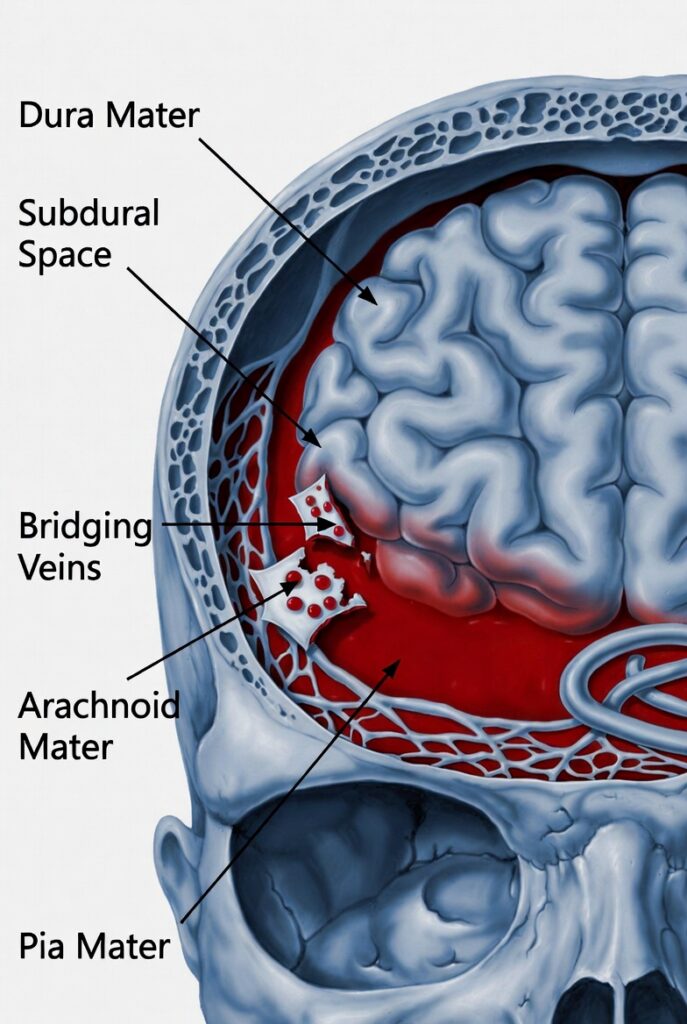
A subdural hematoma (SDH) is a collection of blood that builds up in the subdural space — the area between the dura mater (the tough outer membrane covering the brain) and the arachnoid mater (the next inner layer). This bleeding occurs outside the brain tissue itself but inside the skull, and the accumulating blood puts increasing pressure on the brain.
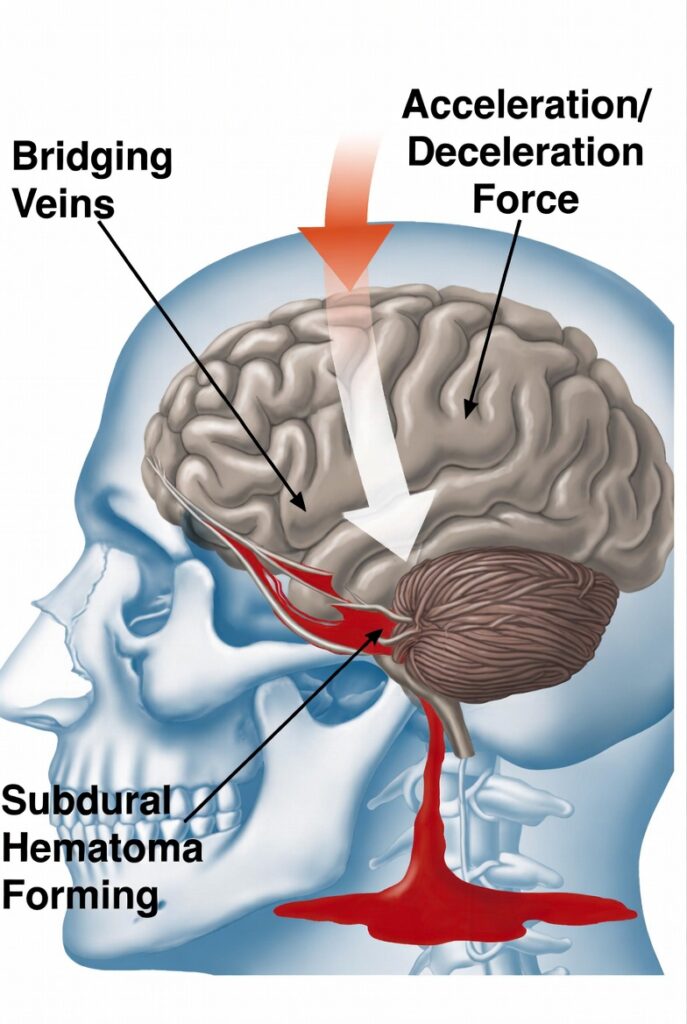
The injury typically results from the tearing of bridging veins — the vessels that drain blood from the brain’s surface into the dural sinuses. When these veins rupture from a sudden impact, violent movement of the head, or rapid acceleration and deceleration forces, blood pools and forms a hematoma that compresses brain tissue and raises intracranial pressure. The consequences can be catastrophic and permanent.
Subdural hematomas occur in approximately 25% of people who suffer serious head injuries, making them one of the most common traumatic brain injuries seen in personal injury cases.
Subdural Hematoma vs. Other Types of Brain Bleeds
People injured in accidents sometimes see multiple medical terms in their records and are not sure how they relate. Here is how a subdural hematoma differs from other types of intracranial bleeding:
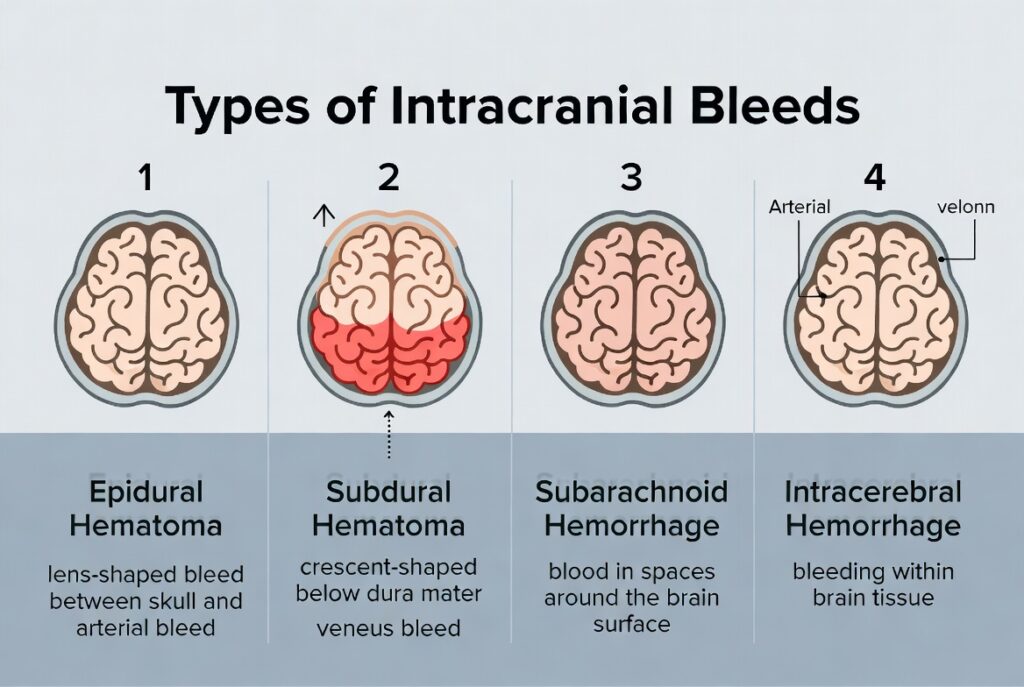
Epidural hematoma — Blood collects between the skull and the dura mater, above the brain’s outer lining. Epidural hematomas are typically caused by arterial bleeding, often associated with a skull fracture, and can cause rapid deterioration. They are anatomically different from subdural hematomas, which occur below the dura.
Subarachnoid hemorrhage — Bleeding in the subarachnoid space, below the arachnoid layer and above the brain surface. These typically involve arterial bleeding and are often associated with aneurysm rupture or severe trauma.
Intracerebral hemorrhage — Bleeding within the brain tissue itself, rather than in the spaces surrounding it.
A subdural hematoma involves venous bleeding in the space below the dura mater. Because venous pressure is lower than arterial pressure, subdural hematomas sometimes develop more slowly than arterial bleeds — but they can still cause severe and permanent neurological damage as pressure gradually increases.
It is also worth noting the distinction between a subdural hemorrhage and a subdural hematoma. A hemorrhage refers to active bleeding. A hematoma is the collection of blood that results. Both terms may appear in your medical records and refer to the same underlying injury at different stages.
Types of Subdural Hematomas
Subdural hematomas are classified by how quickly they develop. The classification affects treatment urgency and prognosis.
Acute subdural hematoma develops within minutes to hours following severe head trauma. It is the most dangerous form. Blood accumulates rapidly, pressure builds quickly, and without emergency treatment the outcome can be fatal. Acute SDH historically carries a mortality rate ranging from 30 to 80 percent, though outcomes have improved with modern trauma care. Emergency surgical intervention is typically required.
Subacute subdural hematoma develops over hours to days or weeks after injury. One of the most dangerous characteristics of subacute SDH is that symptoms can initially appear to improve before worsening as the hematoma expands and pressure increases. This fluctuating pattern delays diagnosis and can cause victims and their families to underestimate the severity of the injury.
Chronic subdural hematoma develops slowly over weeks to months, often after minor or even unnoticed trauma. It is more common in older adults because natural brain shrinkage with age creates more space between the brain and skull, stretching the bridging veins and making them more vulnerable to tearing. Chronic SDH is frequently misdiagnosed as dementia, stroke, depression, or simply “getting older” because symptoms develop gradually — confusion, memory problems, personality changes, and difficulty walking — and the patient may not connect them to a head injury that happened weeks earlier.
All three types can result from accident-related trauma, and all three can give rise to a serious personal injury claim.
Who Is at Risk?
Certain factors increase the likelihood of suffering a subdural hematoma, or increase the severity of one when it occurs:
Age is a major risk factor. In older adults, natural brain shrinkage stretches the bridging veins, making them more susceptible to tearing even from relatively minor impacts. Elderly patients also have more fragile blood vessels, slower healing, and are more likely to be on blood-thinning medications. Infants and young children face elevated risk as well due to the relative size of their heads and weaker neck muscles.
Blood-thinning medications such as warfarin, aspirin, or newer anticoagulants prevent normal clot formation. What would be a minor head injury in a healthy adult can become a life-threatening hematoma in someone on blood thinners.
Prior brain injuries weaken blood vessels and create scar tissue that makes the brain more susceptible to subsequent bleeding. Repeated head trauma over time — from contact sports, prior accidents, or abuse — causes cumulative damage.
Medical conditions affecting blood clotting or vessel integrity, including hemophilia, liver disease, and hypertension, increase risk significantly.
None of these risk factors reduce the liability of a negligent driver, property owner, or employer. If their negligence caused your head injury, they are responsible for the consequences — including any complications made worse by your pre-existing health status.
Common Causes of Subdural Hematomas in Personal Injury Cases
Car accidents are among the most frequent causes. The violent forces of a collision — even at moderate speeds — cause the brain to move within the skull, tearing the bridging veins. Rear-end collisions, T-bone impacts, rollovers, and head-on crashes all generate the kind of sudden acceleration and deceleration that produces this injury.
Uber and Lyft rideshare accidents produce subdural hematomas with the same mechanism as any high-force vehicle collision — but with the added complexity of California’s rideshare insurance framework. During active ride periods, Uber and Lyft maintain $1 million in commercial liability coverage, which is often the difference between adequate compensation and recovery that falls far short of lifetime care needs.
Pedestrian and bicycle accidents involving vehicles tend to produce severe subdural hematomas because the victim has no protection when struck. The head frequently makes direct contact with the vehicle, the ground, or another hard surface, often at high force.
Slip and fall accidents on wet floors, uneven pavement, broken stairs, or unmarked hazards can cause a person’s head to strike the ground with significant force. Property owners have a legal duty to maintain safe conditions for visitors. When they fail and someone suffers a subdural hematoma, they can be held liable.
Workplace accidents — including falls from heights, being struck by falling objects, scaffolding failures, and other construction site incidents — frequently produce traumatic brain injuries including subdural hematomas. These cases may involve both a workers’ compensation claim and a separate personal injury claim against a negligent third party.
Truck and motorcycle accidents produce some of the most severe subdural hematomas. The forces involved are enormous, protective gear has limits, and the resulting brain injuries often require emergency surgery and carry permanent consequences.
Symptoms of a Subdural Hematoma
Symptoms can appear immediately or be delayed by days or even weeks, and they typically worsen as the hematoma expands. Anyone who has suffered a head injury in an accident should be evaluated immediately by emergency medical personnel — even if symptoms seem minor at first.
Common symptoms include:
- Severe or worsening headache
- Confusion, disorientation, or altered mental status
- Drowsiness or difficulty staying awake
- Nausea and vomiting
- Dizziness and balance problems
- Weakness or numbness on one side of the body
- Slurred or slow speech
- Difficulty with memory, attention, or concentration
- Loss of smell or taste
- Sensitivity to light (photophobia)
- Vision changes or unequal pupils
- Personality or behavioral changes
- Seizures
- In severe cases: loss of consciousness, coma, or breathing problems
One of the most dangerous aspects of subdural hematomas is the “lucid interval” — a period after the injury during which the victim feels relatively normal before rapidly deteriorating as the hematoma grows and pressure increases. This is why any head impact in an accident requires prompt CT imaging. Feeling okay at first does not mean you are okay.
In chronic cases, particularly in older adults, symptoms can closely mimic dementia, stroke, or psychiatric conditions. Patients and their families may not connect gradual memory loss, confusion, and personality changes to a fall or accident that happened weeks earlier.
Diagnosis and Treatment
Diagnosis is primarily accomplished through CT scanning, which quickly reveals blood in the subdural space and any compression of brain tissue. MRI provides more detailed imaging and is particularly useful for smaller hematomas or subacute and chronic presentations. Imaging should be repeated when symptoms worsen — as in the case I settled for $6 million, repeat CT imaging the day after admission showed expansion of the bilateral subdural hematomas.
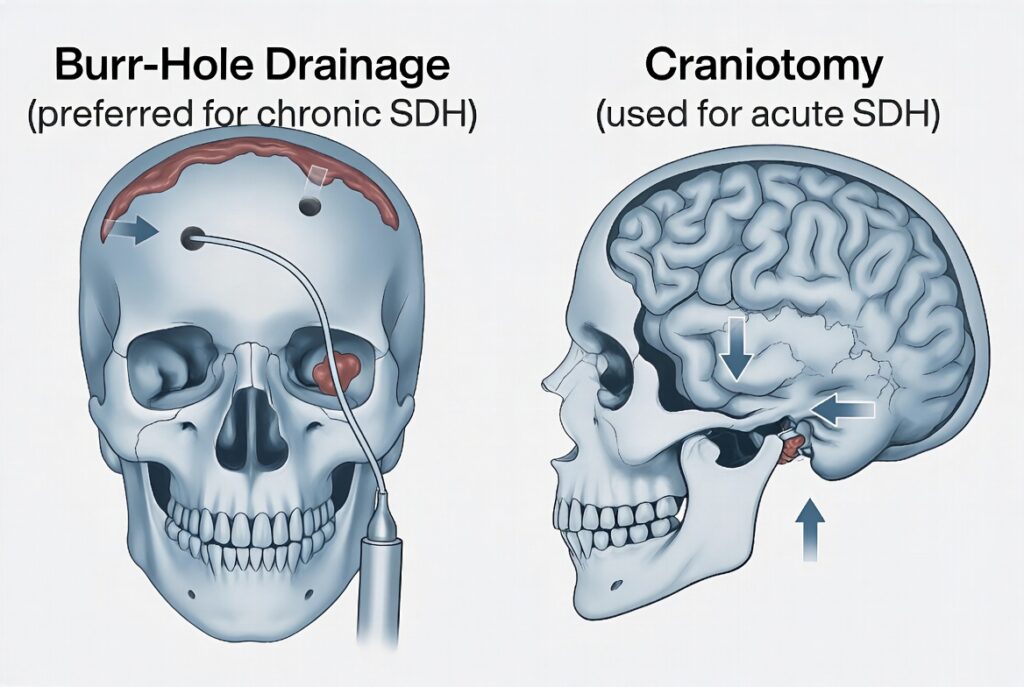
For small, stable, or asymptomatic hematomas, close observation with repeat imaging, seizure medications, and medications to reduce brain swelling may be appropriate. For larger or symptomatic hematomas, surgery is typically required. Burr-hole drainage involves drilling small holes in the skull to drain the collected blood and is the preferred approach for chronic SDH. Craniotomy involves temporarily removing a larger section of skull to evacuate the clot and stop bleeding, and is more commonly used for acute SDH. In some cases, middle meningeal artery embolization may be used to reduce recurrence risk.
Recovery following hospitalization often requires extensive rehabilitation — physical therapy, occupational therapy, speech therapy, neuropsychological treatment, and psychiatric care for PTSD, depression, anxiety, and personality changes that commonly accompany severe brain injuries.
Understanding the Severity: Clinical Tools Used in Brain Injury Cases
When I handle a subdural hematoma case, I work with medical experts who use established clinical tools to document the severity of the injury. Two that frequently appear in medical records and expert reports are worth understanding:
The Glasgow Coma Scale (GCS) measures level of consciousness on a scale of 3 to 15. A score of 15 is normal. A score of 8 or below indicates a severe traumatic brain injury. Scores in the 9–12 range indicate moderate TBI. In the case I settled for $6 million, my client arrived at the emergency room with a GCS of 13 — which, while not the lowest end of the scale, still reflected an injury that produced serious and lasting consequences.
The Rancho Los Amigos Scale is a clinical tool used to rate how people with brain injuries are recovering cognitively and behaviorally. It runs from Level I (no response) to Level X (purposeful and appropriate behavior). A Level V rating means the person responds to simple commands inconsistently, becomes agitated in busy environments, has severely impaired memory, and cannot learn new information. If your loved one has received a Rancho Los Amigos rating, it is important evidence of the severity of their injury and should be part of any damages case.
Long-Term Consequences
Without prompt and appropriate treatment, a subdural hematoma can cause brain herniation — the brain being pushed and displaced — leading to irreversible damage, coma, or death. Even with treatment, many survivors face lasting deficits.
Long-term consequences can include permanent cognitive impairment affecting memory, attention, and problem-solving; personality changes, increased irritability, and impaired impulse control; PTSD, depression, and anxiety; motor function problems including weakness, poor coordination, and balance difficulties; seizure disorders; vision and hearing problems; chronic headaches and fatigue; and in severe cases, significant limitations on the ability to work or live independently.
A subdural hematoma can also cause downstream damage to brain tissue. Encephalomalacia — the softening or permanent loss of brain tissue — can develop in the months following the initial injury, visible on follow-up MRI. When encephalomalacia affects the frontal lobes, it can permanently alter a person’s personality, judgment, impulse control, memory, and emotional regulation.
What a Subdural Hematoma Case Is Worth
There is no standard settlement value for a subdural hematoma case. What a case is worth depends on the severity of the injury, the treatment required, the victim’s age and occupation, the degree of permanent impairment, and the strength of the liability evidence. What I can tell you is that the most important factor in recovering full value is having a lawyer who understands the medicine and is prepared to take the case to trial.
Past and future medical expenses — Emergency care, hospitalization, ICU stays, neurosurgery, rehabilitation programs, neurological monitoring, neuropsychological evaluations, psychiatric care, and medications can collectively reach into the millions of dollars over a lifetime.
Lost wages and earning capacity — A subdural hematoma that causes cognitive impairment, memory deficits, balance problems, or personality changes can make it impossible for a victim to return to their prior work or any competitive employment. A vocational expert and economist calculate the present value of those losses over a working lifetime.
Life care costs — Victims with ongoing medical needs face future care costs that can represent a significant component of damages. These include future neurological monitoring, neuropsychological evaluations, rehabilitation programs, psychiatric care, and any attendant care needs — all of which must be accounted for in a comprehensive damages model.
Non-economic damages — Pain and suffering, loss of enjoyment of life, emotional distress, personality changes, loss of relationships, and the fundamental loss of identity that a brain injury causes are real and compensable. California juries understand brain injury cases deeply, and verdicts in severe cases reflect the full human impact of these injuries.
How I Handle Subdural Hematoma Cases
Brain injury cases require more than legal skill. They require a lawyer who understands the medicine, knows how to work with neurologists, neuroradiologists, neuropsychologists, life care planners, vocational experts, and economists, and who can translate a complex injury into a story that a jury can understand and respond to.
I approach every subdural hematoma case by building the full picture from the beginning. That means obtaining all imaging and medical records immediately, retaining the right experts early, documenting the daily impact on the client’s life and relationships, and constructing a damages model that captures every consequence of the injury — past, present, and future. I do not settle these cases for less than they are worth, because I understand what they are worth and I am prepared to try them.
I have recovered over $25 million for injured clients over the course of my career, including a $6,000,000 settlement for a client who suffered bilateral subdural hematomas, a skull fracture, and permanent traumatic brain injury after being struck by a vehicle in a crosswalk.
How Insurance Companies Defend Subdural Hematoma Cases
If you have been seriously injured, you need to understand something before you hire a lawyer or accept any offer: the insurance company defending this case has a playbook, and they run it in every serious brain injury case. I have seen it from the other side of the table. Here is how it works.
They call it a “minor” injury regardless of the evidence. Even when a client has bilateral subdural hematomas, a skull fracture, an ICU admission, and permanent brain tissue loss confirmed on MRI, the defense will characterize the injury as “minor” in every document they file. The goal is to set a tone — to the mediator, to opposing counsel, and eventually to a jury — that the injury is being exaggerated. They do this no matter what the imaging shows.
They hire their own neurologist to contradict your doctors. Insurance companies retain defense-friendly neurologists and psychiatrists to conduct what is called an Independent Medical Examination, or IME. The name is misleading — these are not independent examinations. The doctor is hired and paid by the insurance company, often meets with the patient for one to two hours, and produces a report designed to minimize the injury. In the cases I handle, I have seen defense neurologists conclude that a client with documented encephalomalacia on MRI and an ICU admission was “overstating his problems” and that his symptoms were really due to “underlying emotional issues.” That opinion was used to argue the client could return to work and did not need ongoing care.
They use a neuropsychologist to attack your test results. One of the most common and effective defense tactics in TBI cases is to administer neuropsychological testing and then argue that the injured person did not put forth their best effort — which renders all the results invalid. Defense neuropsychologists use what are called validity or effort tests embedded within larger cognitive batteries. If they can show poor performance on effort measures, they argue that none of the cognitive deficits are real or measurable. This tactic can effectively neutralize your own neuropsychological expert’s findings.
They dig up your medical history looking for pre-existing conditions. Before the insurance company makes any serious offer, they will subpoena every medical record you have ever had. They are looking for prior treatment for depression, anxiety, headaches, neck pain, back pain, dizziness, memory problems — anything that overlaps with your current symptoms. They will argue that your complaints today are not the result of the accident but are instead a continuation of pre-existing conditions. In California, this does not eliminate your claim — you are entitled to recover for any aggravation of a pre-existing condition — but it complicates the damages picture and gives the defense a basis to minimize what they owe you.
They watch what you do and use it against you. Insurance adjusters and defense attorneys pay close attention to everything an injured person does after an accident. If you drive a car, coach a youth sports team, tend a garden, or travel to visit family, those activities will appear in defense filings as evidence that you are not as injured as you claim. The answer to this tactic is not to stop living your life — it is to have a lawyer who can put those activities in proper medical context and explain what the client can and cannot do and why.
They attack the life care plan. If your experts have produced a life care plan projecting future medical costs, the defense will challenge every line of it. They will argue the projections are speculative, that you do not actually need certain treatments, and that your current functional level does not support the projected care needs. Their own life care experts will produce competing projections at a fraction of the cost. Getting full value for future care requires a life care planner whose methodology is airtight and a lawyer who can expose the weaknesses in the defense’s analysis.
They argue you failed to mitigate your damages. If you missed appointments, did not complete a recommended rehabilitation program, or delayed treatment for any reason — including lack of insurance or language barriers that limited your access to care — the defense will argue you failed to mitigate your damages and that some portion of your harm is your own responsibility. I know how to address this argument and what it takes to neutralize it.
They challenge your medical bills under Howell v. Hamilton. Under California law, you are generally entitled to recover only the amount actually paid for your medical care, not the full amount billed. Defense attorneys use this to dramatically reduce the apparent value of your medical damages, particularly when providers have accepted discounted rates. This requires careful economic analysis and, in some cases, expert testimony on the reasonable value of the treatment provided.
Understanding this playbook is why experience matters. I have handled serious brain injury cases against these arguments repeatedly. I know what the defense is going to do before they do it, and I build the case from day one to withstand it.
Frequently Asked Questions
In most personal injury cases in California, you have two years from the date of injury to file a lawsuit. There are important exceptions — cases involving government entities may require you to file a government tort claim within six months of the incident. I recommend contacting me as soon as possible after any accident so that evidence is preserved and no deadlines are missed.
Delayed symptoms are common with subdural hematomas, particularly subacute and chronic forms. A gap between the accident and your diagnosis does not eliminate your claim. What matters is that the injury is causally connected to the accident, which medical records and expert testimony can establish. Do not assume delayed diagnosis means you do not have a case.
California follows a pure comparative fault rule. Even if you were partially at fault for the accident, you can still recover damages — your recovery is reduced by your percentage of fault, but it is not eliminated. Do not assume that partial fault bars your claim.
Uninsured and underinsured motorist coverage, employer liability, property owner liability, and other sources of recovery may be available depending on the circumstances. I evaluate all potential sources of compensation in every case I take.
No. The value of a case turns on the impact the injury has had on your life, not on whether a craniotomy was performed. A subdural hematoma managed without surgery can still cause significant cognitive deficits, personality changes, lost wages, and ongoing medical needs — all of which are compensable.
The terms are often used interchangeably. Technically, a hemorrhage refers to active bleeding while a hematoma refers to the collection of blood that results. You may see both terms in your medical records — they refer to the same underlying injury at different stages.
An epidural hematoma occurs between the skull and the outer surface of the dura mater, and typically involves arterial bleeding associated with a skull fracture. A subdural hematoma occurs below the dura mater, involves venous bleeding from torn bridging veins, and can occur with or without a skull fracture. Both are serious traumatic brain injuries.
Contact a San Francisco Subdural Hematoma Lawyer Today
If you or a family member suffered a subdural hematoma in an accident caused by someone else’s negligence, I want to hear from you. I offer free consultations, I work on a contingency fee basis, and I have the experience and resources to handle serious brain injury cases from investigation through trial.
Call me at (415) 851-4557 or fill out the contact form on this page. I represent injured clients throughout San Francisco and the Bay Area.